Why cholesterol isn't the villain — and what actually predicts your risk
For years, cholesterol has been portrayed as a ticking time bomb — a fat-like substance silently clogging your arteries. The narrative is simple: high cholesterol equals high risk. But the science, as usual, is not.
In reality, cholesterol is essential to human health. Every cell membrane in your body contains it. It’s a building block for testosterone, estrogen, cortisol, and vitamin D. Your brain is about 20% cholesterol by weight. You can’t survive without it.
So why the bad reputation?
Because cholesterol travels in the blood — and how it travels matters far more than its total volume.
What You’re Actually Measuring: Lipoproteins, Not Cholesterol
Most people are shocked to learn that the “good” and “bad” cholesterol numbers on a lab test aren’t cholesterol at all. What you’re actually seeing is the amount of cholesterol carried inside specific types of proteins called lipoproteins.
Think of cholesterol as a passenger and lipoproteins as the cars carrying it through your bloodstream.
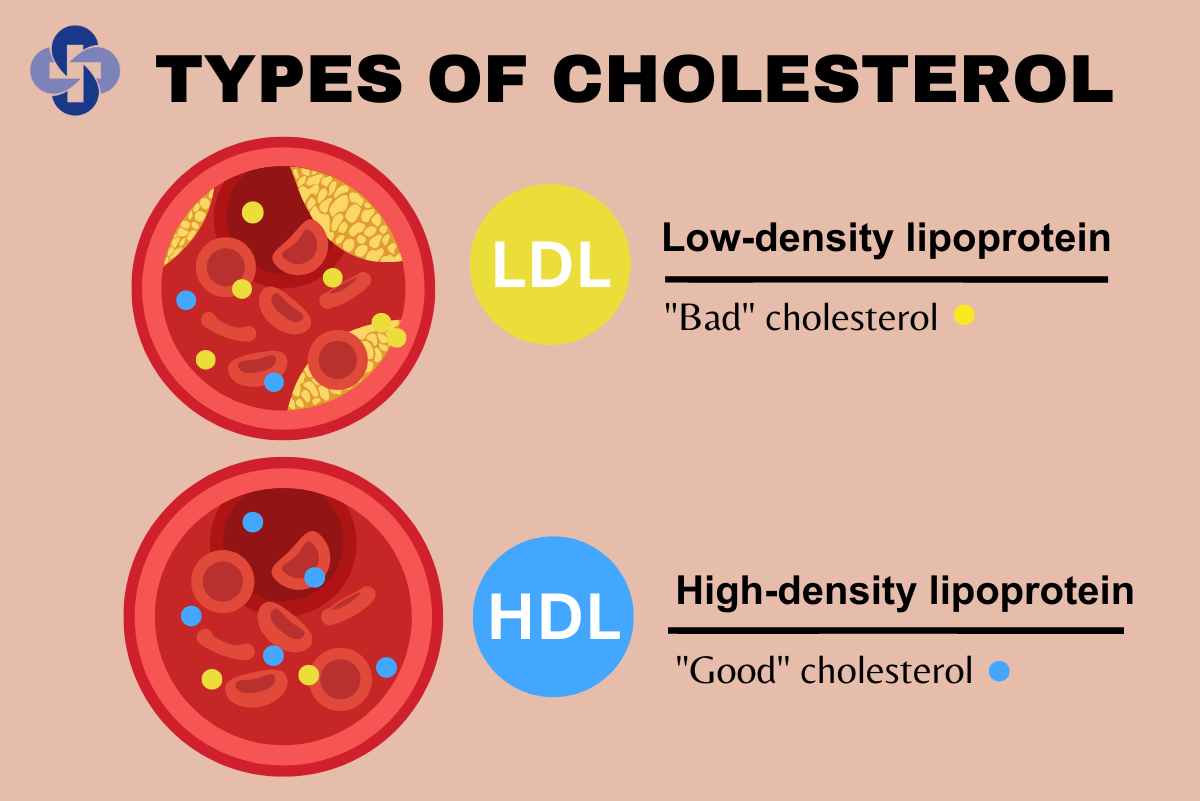
- LDL (Low-Density Lipoprotein): Delivers cholesterol to cells. Often labeled “bad” because high levels — especially small, dense particles — can lodge in arterial walls and trigger inflammation.
- HDL (High-Density Lipoprotein): Transports excess cholesterol back to the liver for clearance. Called “good” because it helps clear the system and maintain lipid balance.
But even that good/bad framework is outdated. What matters more is how many of these particles you have, how well they function, and how inflamed your system is.
Total Cholesterol Doesn’t Predict Much — Here’s What Does
For decades, physicians looked at total cholesterol as a stand-alone marker for cardiovascular risk. But mounting research has shown that total cholesterol doesn’t tell us enough. A high LDL level might not be risky at all if your particle size is large and buoyant, your inflammation is low, and your HDL is active and functional.
Here are the biomarkers that actually matter:
ApoB (Apolipoprotein B)
ApoB is a direct measure of the number of atherogenic particles (mostly LDL and VLDL) in your bloodstream. Each of these particles contains one ApoB protein — so ApoB tells you how many cholesterol-carrying particles are present.
High ApoB = more vehicles capable of penetrating arterial walls.
Triglyceride:HDL Ratio
This ratio is a powerful predictor of insulin resistance and metabolic dysfunction. A ratio under 2:1 (mg/dL) is optimal. If your triglycerides are high and HDL is low, your body is likely struggling to regulate blood sugar and manage inflammation.
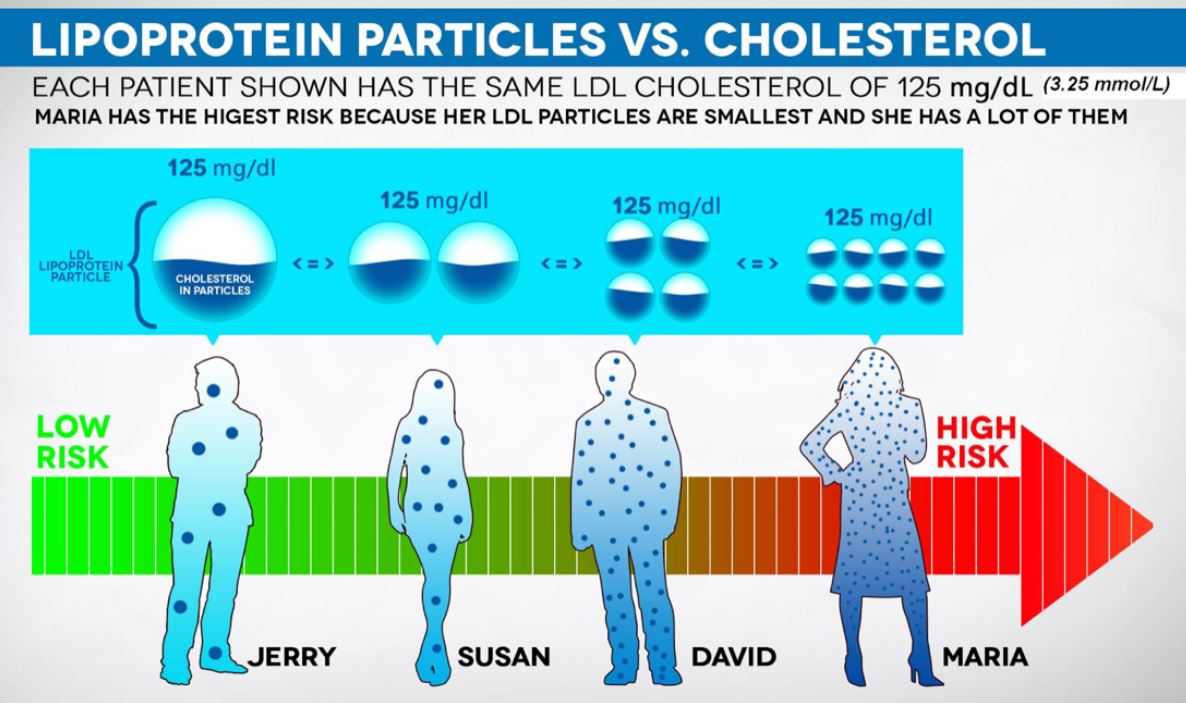
LDL Particle Size and Number
Not all LDL is equal. Small, dense LDL particles are more likely to oxidize and inflame arteries. Large, buoyant LDL particles are far less atherogenic. An advanced lipid panel (like NMR) will show whether your LDL is high-risk or benign.
Inflammation Markers (e.g., hs-CRP)
High-sensitivity C-reactive protein (hs-CRP) is a marker of systemic inflammation — a known contributor to plaque rupture, endothelial damage, and clot formation. Even with ideal cholesterol levels, high CRP elevates your cardiovascular risk.
Why Cholesterol Still Matters — But In Context
You still need to measure cholesterol, but in context with metabolic health, blood sugar regulation, and inflammation.
For example, two people could both have an LDL of 140 mg/dL:
- Person A: Active, lean, low insulin, large LDL particles, low ApoB, low CRP. → Low real-world risk
- Person B: Sedentary, insulin-resistant, high triglycerides, high ApoB, elevated CRP. → High risk despite same LDL
This is why comprehensive testing is crucial. Cholesterol doesn’t exist in a vacuum — it’s one part of a larger metabolic picture.
A Note on Statins and Medication
If you have very high LDL, a genetic condition like familial hypercholesterolemia, or a history of cardiovascular disease, your doctor may recommend statins or other lipid-lowering medications. These can reduce ApoB levels and event risk in high-risk individuals.
But even then, medication doesn’t replace lifestyle. The most protective outcomes come from combining pharmacology with consistent training, smart nutrition, and inflammation control.
Actionable Insights
- Don’t rely on standard panels: Ask for an ApoB, LDL particle analysis (via NMR), triglyceride:HDL ratio, and hs-CRP.
- Track your response: Get re-tested every 6–12 months to see how your lifestyle changes affect key markers.
- Exercise strategically: Combine strength training with low-intensity cardio to shift lipid metabolism long-term.
- Go beyond food myths: Dietary cholesterol isn’t the problem. Focus on blood sugar, inflammation, and food quality.
- Know your context: One-size-fits-all cholesterol targets ignore personal risk factors like age, genetics, insulin resistance, and inflammation.
The Bottom Line
Cholesterol is not the enemy — context is everything. It’s the number, size, and behavior of your lipoprotein particles, combined with your metabolic and inflammatory status, that truly dictate risk.
By shifting the focus away from fear and toward precision, you give yourself the tools to not just manage cholesterol — but use it as a marker of strength, resilience, and long-term performance.



